
I am dedicating this post to the writers, directors, and long-term cast of Grey’s Anatomy. Simple because I’m fairly certain I’m living a storyline you have somehow missed despite twenty-two seasons.
If you’re new here, hey! I’m Lucy. A 28-year-old who has been something of a medical mystery for over 12 years now. For some reason, my body likes collecting chronic conditions like they’re Pokemon! Whilst I can think of greater things to be achieving in my 20s, if some good can come from me yapping about my experiences then I’d say that’s a win!
Throwing it back to 2018 …
2018 witness the unlocking of a brand new specialty in my collection. That’s correct, the following symptoms landed me in the consultation room of a rheumatologist:
- Mystery headaches
- Crippling fatigue
- Obscure breathing issues
- (Apparently) imaginary stomach pains
- Unexplainable bruising
- Rapid heart rate
- Painful joints
The list of symptoms didn’t end there, but these were the main ones. Frustratingly, they saw me dismissed by:
- GPs
- Neurologists
- Cardiologists
- Gastroenterologists
- Respiratory consultants
At that stage, the rheumatologist was simply a tick box exercise. My GP was crossing off specialties in order to justify a psych referral. In the appointment, I reeled of my ever-growing list of symptoms. The found myself subjected to the rheumatology examination.
I remember this involving a lot of bending my joints in ways I apparently shouldn’t be able to. In my defence, I was a former dancer and gymnast. Of course I was flexible! He completed his examination by asking me to place my hands flat on the floor (I could). Then, he awarded me a score of 9/9 on the Beighton scale.
Surely full marks was the aim?! …
I had no clue what this meant, but surely full marks was the aim?! Apparently not, but what can I say, I’ve been a medical overachiever from day 1! I will hasten to add that despite being unimpressed with my high score, he didn’t elaborate on why. Instead, he told me I would have problems when I got older, most likely in the form of arthritis.
I think about this conversation on an almost daily basis. In that moment I confidently imagined older meaning past 50.
More on that later …
As for the other symptoms, he had very little to say on those matters and like the others, batted the responsibility back to the GP. The worst part of all being clueless as to just how significant it was being hypermobile. Disclaimer: there are several forms of hypermobility including benign hypermobility. So much so that I never remembered to mention it as a diagnosis when reeling off my medical history!
Fast forward to 2024 …
2024 was going to be a good year. I’d recovered from my laparoscopy which saw me diagnosed with endometriosis across multiple organs in my abdomen. I was also almost 18 months into receiving cranial botox for mystery headaches. There was one thing I didn’t factor in … a headache to step in and derail my life in the afternoons.
It took me roughly 2 weeks to associate lying flat with freeing me of the headache. Then, several more days before deciding that probably wasn’t normal!
The initial diagnosis …
Remember that irrelevant until I get older hypermobility diagnosis? Well, it was about to enter the chat! Nearly three weeks after the headache started, my mum and I ended up back in neurology outpatients. It was the hospital I’d been under since 2019. Within that on the small side consultation room also sat my neurologist, one of his registrars, and my headache nurse specialist.
If you would like to read more about that consultation, I will link my previous post here, but their examination led to the same conclusion. A spinal CSF leak. My consultant neurologist went on to ask if I’d ever been told I was hypermobile. In potentially the most nonchalant way witnessed I responded: Oh yeah ages age, they scored me 9/9 on whatever the scale is they use!
Yet again, the excitement was not mutual on both sides. Unfortunately, the questions that followed I couldn’t answer because the rheumatologist back in 2018 had never elaborated any further beyond “you are very hypermobile.”
This is where it gets interesting …
I underwent my first epidural blood patch roughly 4 weeks after first noticing the headache. Now, for anyone who is unfamiliar with a blood patch, they leave you in trendelenburg position for 6 hours post procedure. Click here for a more detailed account. However, when they allowed me to get up, I was completely headache free.
At the time I consented to admission, they assured me complete relief from headaches was possible in the future. Furthermore, being completely headache free implied successful blood patching, and confirmed the diagnosis of a spontaneous spinal CSF leak.
All wrapped up and done …
That was that. Symptoms, diagnosis, and treatment all wrapped up and done in 4 weeks on the NHS. Nothing more could be said beyond incredible service. Well, that was until the headache returned. I suppose the relief was nice while it lasted.
Naturally, the blood patch blowing was the obvious explanation. This being potentially thanks to my already weak connective tissue (thank you hypermobility).However, my neurologist felt in that moment that a second blind blood patch was pointless and instead they should attempt a CT myelogram (a scan used to look for CSF Leaks).
The CT myelogram came back clear, and frustratingly my neurologist was on annual leave. This meant the next steps conversation took place with the on call neurologist. The myelogram could have been clear for one of two reasons:
- There is no active leak in spite of my symptoms.
- There is a leak, but is it a fistula leak and therefore not identifiable on conventional myelography.
That remained the million dollar question nobody could answer. With limited options available, the on call consultant recommended a second blind blood patch (again, click here for the full story). I was skeptical, but you trust the specialists right?
I was right to be skeptical …
That blood patch was a pivotal moment, but not for the right reasons. This blood patch didn’t work in any manner of speaking. What it did do was leave me with crippling spinal pain and simultaneously activate a whole heap of generic symptoms.
I wholeheartedly wish I had trusted my gut feelings. Even now, I can pinpoint this as the moment everybody began to become distant. Appointments became more sporadic. My once believed symptoms started to become dismissed. They passed me from consultant to consultant in various parts of the country, but nobody really took an interest.
In the meantime, I began to experience the following symptoms either for the first time, or in a worsening manner:
- 24/7 nausea to the point where I was consuming 200-500 calories on a good day.
- Fatigue to a level where moving any part of my body compared to lifting tonne weights.
- Random flushing or hives most notably on my neck and chest.
- Brain fog on a scale where I couldn’t remember things I previously would never forget.
- Reemerging chest pain and tightness that had resolved 6 months prior.
- General, non-descriptive pain in multiple joints.
- Abdominal pain and bloating (again symptoms I had been previously free of for several months)
- Throat itching and periods of feeling congested.
- Episodes of palpitations but normal cardiac workup.
If I wanted answers, I would have to find them …
18 months passed between that second blood patch and this moment. By this point, I weighed just 45kg (7st). This made me not only severely underweight, but the most underweight I had ever been. No matter the anti-sickness medication prescribed, nothing even touched the edges of the nausea. Realistically, I could safely confirm the nausea as the most debilitating symptom. When I think about it, this is crazy considering the headache never lessened.
I relentlessly pushed through necessary day-to-day activities, but the outcome was always the same. A flare up severe enough to incapacitate me completely for 5 to 7 days, or worse, a hospital admission. It became a vicious chuckle that nobody cared about breaking. Instead, the narrative changed from belief to doubt.
They replaced belief with doubt about the leak, without offering a plausible alternative. Instead, I found myself pushed back down the mental health route. The belief that once flourished became doubt topped with clouds of questions hanging over me. Maybe I didn’t still have the leak, but equally the plethora of symptoms I continued to experience were not psychological.
The deep, dark depths of Dr Google …
I told myself there must be an answer somewhere. I couldn’t be the first person in the world to experience this pattern of symptoms. It took me a while, but somewhere towards the beginning of October 2025, I found a brand new research article from the US.
Disclaimer: All of the following is based on my own interpretation and theorisation of the information I read …
This article introduced me to the condition Mast Cell Activation Syndrome or MCAS for short. As a condition, I knew practically nothing about it, but I had spare time to learn!
This is where it starts to become a bit confusing, but I promise reading to the end is worth it …
Mast Cell Activation Syndrome (MCAS) …
MCAS is a condition whereby the mast cells, which are immune cells, release an excessive amount of inflammatory chemicals. This is in response to various triggers. Mast cells are found in all the tissues of the body and can be involved in:
- Allergies
- Asthma
- Skin disease
- Brain inflammation
- Cardiovascular issues and more …
The release of these chemicals causes a variety of allergy-like symptoms that are often very generic. Furthermore, because these cells are present in so many tissues, activation of them can cause a wide range of symptoms in different areas of the body.
The symptoms themselves can be acute, including anaphylaxis, or they can be chronic. Any individual can have any combination of these issues, and they can change over time. Below are a few of the more typical symptoms of MCAS.
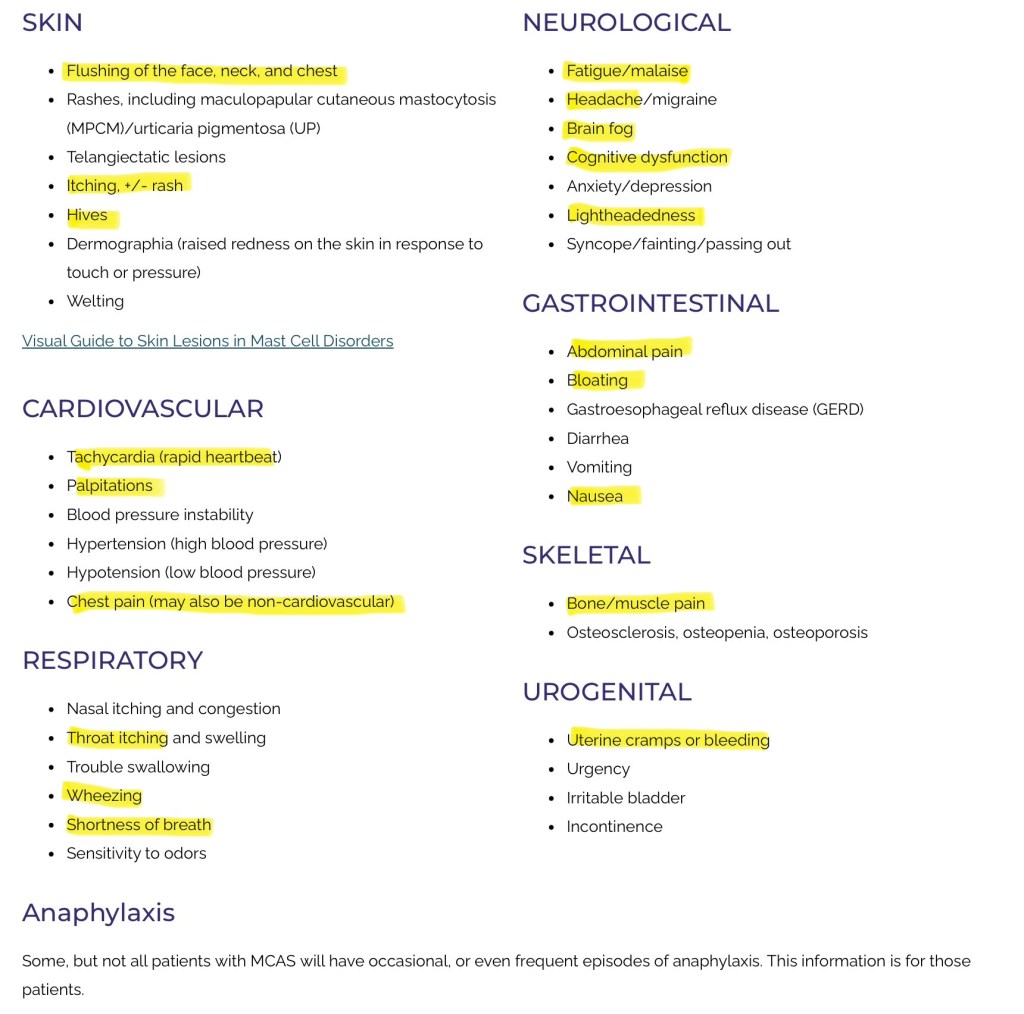
As you can see, the highlighted symptoms all emerged post that second blood patch. At this stage, 18 months since first developing the headache, nothing could be a coincidence in my eyes.
Is this really all relevant!? …
So what exactly does this have to do with my positional headache that may or may not still be due to a spinal CSF leak?
(To recap the above disclaimer … the following is not medical advice in any manner. It is simply my own interpretation and theorisation).
Apparently, the MCAS rabbit hole I fell down could be very relevant to my positional headache. Particularly in light of the fact my apparently unproblematic hypermobility is anything but that. In fact, my unproblematic hypermobility passed the hypermobile Ehlers-Danlos Syndrome (hEDS) diagnostic criteria with flying colours.
Back to THAT research paper …
This research paper in question was titled Mast cells regulate brain-dura interface and CSF dynamics. It contained a lot of words in there that definitely went over my brain fog ridden head, but some of the revelations left my jaw firmly on the floor!
The core idea presented in the research paper is that mast cells (a type of immune cell) are collect in high volumes in the dura (mater). More importantly, they are key regulators of CSF dynamics and critically help to control how cerebrospinal fluid flows in and out of the brain.
My previous research already confirmed an understanding of how mast cells rapidly release histamine upon activation. The key piece of information is that this released histamine leads to vasodilation (widening) of bridging veins. When this happened, CSF flow is temporarily reduced and intracranial pressure decreases.
Let’s say that again … Acute mast cell activation decreases intracranial pressure …
I already knew from the previous 18+ months that decreased (or low) intracranial pressure presented as a positional headache that relieved upon lying down! When mast cells stay chronically activated, they can interfere with CSF flow. Over time, this can contribute to cognitive problems as toxins build up.
So what does this mean? …
In theory, it means MCAS could:
- Mimic CSF leak symptoms and explain why individuals have “low pressure headaches” but no visible leak on the imaging.
- Alter pressure regulation in the same was CSF Leaks do.
- Chronic activation of these mast cells can weaken connective tissues due to the exposure to constant histamine. Over time this may cause micro tears (spontaneous leaks).
Therefore, there is the possibility that first blood patch actually did seal my spontaneous leak, but at the same time activated potentially pre-existing (and underlying) MCAS.
Moving forwards …
Again, this is all hypothetical with the potential to be crossing the border into delusional. However, after picking my jaw up off the floor, I began taking an over-the-counter form of fexofenadine (an antihistamine). I did this each morning and the benefits were unreal.
The nausea, which had been one of the most debilitating co-existing symptoms, practically disappeared after a few days. Gradually, over the subsequent few weeks, my calorie intake almost tripled. Disclaimer: this was managed by a licensed dietician to avoid refeeding syndrome. As a result, I began to put on weight for the first time in nearly 2 years.
The positional headache …
Despite the revolutionary breakthrough with the crippling nausea, the fexafenodine had no impact on the low pressure headache. At present, the NHS can’t agree in MDTs on whether I do, or do not still have a leak. Whilst this continues, I’ve decided to take a side quest down the MCAS medication path.
In theory, if the MCAS was activated by the blood patch, then the appropriate medication combination could at least have the potential to reduce the severity of the headache without the need for more needles entering my spine.
Something about me is no matter how poorly I feel, when I get an idea in my head I’m going to follow it through. Therefore, I managed to secure an appointment (privately) with an MCAS specialist on the 10th March 2026. One thing is for certain. After the most horrific post-blood patch experience back in April 2024 alongside an equally horrific CT Myelogram in May 2024, the last thing I want is more needles in my spine if medication is an option!
Stay tuned for the outcome! …
Wow, that ended up being so much longer than I expected! I’ve been a medical mystery for so much longer than the 2 years I’ve been leaking (or not). In this time, all too often been on the receiving end of dismissal on the grounds of something being unlikely. If my past has taught me anything, it’s that rare and unlikely are key words for it happening to me!
Keep reading over the next few months and beyond! Hopefully, to find out if I do still have a spinal CSF leak, or if the MCAS is mimicking the symptoms of a spinal CSF leak!
May your symptoms be believed and your specialists be competent.
Your favourite headache x
Discover more from Not just a headache, honey
Subscribe to get the latest posts sent to your email.
One thought on “Connecting the clues: Plot line for Greys Anatomy S23”